Social capital and health among participants in the cachibol league in Israel
תאריך: 10/5/2021
Orna Baron-Epel, Deborah Kadish - University of Haifa, Israel
The Israeli cachibol league, Mamanet, is a grass roots non-professional community sports club for mothers. Our aim was to assess if participants in the Mamanet League have higher levels of social capital and if social capital and wellbeing improve with time. Two groups were interviewed: a control group not participating in the league and a group of Mamanet participants. The women were interviewed within 3 months of joining (T1) and 13–15 months later (T2). The questionnaire included questions on sociodemographic characteristics, social capital (social support, social involvement, trust) and wellbeing (self-reported health (SRH), psychosomatic symptoms, depressive symptoms). At T1 the participants had higher social capital and SRH scores than the control group and lower psychosomatic and depressive symptoms compared with the control group. Participation in the Mamanet League seems to improve two of the three social capital measures: social support and social involvement, showing an increase among the Mamanet group over time and no change in the control group. Participation in the
Corresponding author:
Orna Baron-Epel, School of Public Health, Faculty of Social Welfare and Health Sciences, University of Haifa, Mount Carmel, Haifa 31905, Israel.
Email: ornaepel@research.haifa.ac.il
2 International Review for the Sociology of Sport 00(0)
league had no significant effect on wellbeing during this period. Women that participate in sports clubs may initially have higher social capital; in addition, participation may increase levels of social capital over time.
Keywords
gender, Putnam, self-reported health, social capital, social involvement, social support, trust, wellbeing, women’s sports
Introduction
The importance of physical activity for overall wellbeing has been well documented. However, the exact nature of the activity, as well as the best way to achieve compliance with physical activity recommendations, is still being studied. Physical activity can be performed individually or in groups and teams; when a competitive component is added to the activity, it is coined as “sport.” Some research suggests that conscious participation in sports (versus less organized physical activity) has been associated with better mental and other health outcomes (Andersen et al., 2019; Marlier et al., 2015; Ottesen et al., 2010). Moreover, there is still a debate whether social aspects of participation in organized sports, such as social capital, add to health and wellbeing (Coll-Planas et al., 2017; Okayasu et al., 2010). Evidence is scarce regarding the effects of participating in such groups of homoge neous or non-homogeneous individuals on various aspects of social life and wellbeing. Some research does exist regarding being active in sports clubs, but usually not in compari
son to people that are not active in sports clubs. Therefore, in this study we chose to research the Israeli cachibol league as a case study that can answer these questions among women. In this study we ask to what degree do women whoe participate in sports clubs have better social capital and wellbeing, and whether participation increases these variables.
Social capital
Current conceptualization of social capital is based on three scholars, Pierre Bourdieu, James Coleman and Robert Putnam, who elaborated on the concept during the past 40 years (Bourdieu, 1986; Coleman, 1988; Putnam, 1993, 1995). A large body of literature has analyzed the theoretical aspects of these three leading figures and can be found else
where (Baron et al., 2000; Bartkus and Davis, 2010; Field, 2003; Johnston and Percy Smith, 2003; Lewandowski, 2015; Numerato, 2008).
Coleman’s conceptualization of social capital is based on the individual, micro-level. His conceptualization focused on the interdependencies between people (Coleman, 1988). On the other hand, Pierre Bourdieu defined social capital based on power in social class. Bourdieu focused on the social group as a whole, including a meso-level analysis. Members have to be actively engaged, developing useful relationships (Bourdieu, 1986).
Robert Putnam’s conceptualization of social capital is situated at the macro and political level, proposing that participation in structured networks, such as sports clubs, enables civic engagement and improves society’s efficiency (Putnam, 1993, 1995). Drawing on Coleman, Putnam’s social capital is an umbrella term that draws together relationships within net
works, norms of reciprocity, mutual support and trustworthiness (Feldstein and Putnam,
Baron-Epel et al. 3
2003). As Putnam indicated, “networks of civic engagement foster sturdy norms of general ized reciprocity and encourage the emergence of social trust” (p. 67). Bourdieu and Coleman suggested that social capital is a rational individual action (Bourdieu, 1984, 1986; Coleman, 1990), whereas Putnam’s conceptualization of social capital is of a more productive, sup portive, trusting and effective society, for the benefit of a wider population. This later con ceptualization has garnered increased support in the literature (Welty Peachey et al., 2013).
Simply put, Putman suggests that “social networks have value” (Putnam, 2000). Social networks that exist within a society enable social ties to build trust and reciproc ity; people can cooperate and work toward shared objectives (Putnam, 1996). In Putman’s view, social networks rich in social capital can simultaneously provide “good” for the individual and the community; this “good” can include material resources, opportunities and emotional support, leading to better quality of life and health that benefit individuals and societies. Putman’s conceptualization of social capital was chosen for this study as it positions participation in structured networks, such as sports clubs, as enhancing a pro ductive, supportive, trusting and effective society, for the benefit of a wider population.
In this study we chose to adopt Putman’s definition of social capital: “features of social organization such as networks, norms, and social trust that facilitate coordination and cooperation for mutual benefit” (Putnam, 1995, 2000).
One of Putnam’s additions to the theory of social capital was the definition of bond ing, bridging and linking social capital. Bonding social capital is built on trust between like-minded individuals (Putnam, 2000); this type of social capital is especially strong in participation in sports clubs (Elmose-Østerlund and van der Roest, 2017). Bonding capi tal is often associated with “cognitive” social capital, where psychological support rather than material support plays a central role. This study assesses bonding capital among women belonging to a cachibol sports club.
Putman suggested five indicators for social capital: (1) social involvement, (2) politi cal involvement (participating and attitudes), (3) volunteering and reciprocity, (4) trust, and (5) social support. Social capital has been suggested to encompass both structural and cognitive dimensions (Harpham, 2002). The current study measures three cognitive social capital indicators hypothesized to be associated with participation in sports groups: social involvement, trust and social support. Social trust is a key in Putnam’s conceptu alization of social capital. In Putnam’s writings social trust reflects the trust people hold toward members of society in general (Elmose-Østerlund and van der Roest, 2017).
As this study involves women, we think it is important to view social capital through a gender lens as voluntary work is perceived more as the domain of women and sports more as the domain of men (Forsdike et al., 2019; Gidengil and O’Neill, 2006). Therefore, studying social capital among women in sports can add to the social capital debates. The connectedness with others is central to women, and the development of their identity and self can be enhanced by social capital; this has been suggested to improve their mental health (Forsdike et al., 2019; Gidengil and O’Neill, 2006)
Social capital and sports
Putnam’s version of social capital has been popular among sport researchers (Harvey et al., 2007; Welty Peachey et al., 2013). Higher social capital is associated with partici pation in organized sports; participation seems to contribute to generalized trust, more
4 International Review for the Sociology of Sport 00(0)
social connections, and more social activity. It is theorized that these benefits are a result of the transfer of information (both social and political) between participants, the social influence that members have on one another, and a shared identity working toward a common goal (Seippel, 2006). Sports, then, can provide the environment for the devel
opment of relationships within communities that could lead to an increase in social capi tal (Sherry et al., 2011; Smith and Westerbeek, 2014). Sports can also provide connections between diverse groups and social networks (Burnett, 2006), as well as foster social inclusion and social mobility for disadvantaged peoples; this provides opportunity to make friends and develop networks, reducing social isolation (Jarvie, 2003; Sherry, 2010; Spaaij, 2009). Settings that encourage team (versus individual) sports and include a wide range of members seem to be associated with higher levels of social capital, as opposed to sports settings that are more exclusive (Okayasu et al., 2010).
Exploring social capital through women’s sport participation may illuminate a particu lar gendered experience (Osborne et al., 2009). Women’s participation in team sports was found to be more significant to the development of social capital when compared with participation in individual sports such as running (Ottesen et al., 2010). In addition, women living in neighborhoods with higher levels of trust in their peers were more likely to engage in physical activity (Ball et al., 2010). The potential benefits of bonding and cognitive social capital may be more pronounced for women, as these concepts support the impor tance of women’s informal social interactions (Ferlander et al., 2016; Pahl, 2000). A study of US college athletes found that women playing team sports held more social capital than those playing individual sports and men playing team sports (Clopton, 2012). Clopton sug gested that women found “communal values” in belonging to a team and that social capital derived from team sports benefited women more than men because of their ability to sus tain deeper and more meaningful relationships over time (Clopton, 2012). However, wom en’s experiences of social capital within sports are still relatively unknown.
Although significant associations have been found between sports participation and social capital, a directional relationship cannot currently be absolutely established. One perspective asserts that participation in sport does not create social capital among the participants where previously less or none existed, but it is rather that sport groups reproduce and reinforce exist
ing patterns of social capital among the participants (Lewandowski, 2018). It has been sug gested that individuals who participate in group sports have higher levels of social capital, compared with those who participate in individual physical activity, to begin with (Andersen et al., 2019; Bailey et al., 2013; Ottesen et al., 2010). What is unclear is whether an existing higher level of social capital is a pre-requisite for individuals to participate in such sport teams, or whether it is the participation in the sport or team that increases social capital. Studies to date have been unable to verify which is the case. Perks (2007) suggested that sports activities do have the capacity to increase social capital. Specifically, community sport clubs were suggested to have the ability to nurture social capital (Okayasu et al., 2010).
Social capital and health
Putnam, in his seminal book “Bowling alone” devoted a chapter to health in which he summarized previous research starting with the nineteenth century Emile Durkeim (Putnam, 2000). He suggests that “social connectedness is one of the most powerful
Baron-Epel et al. 5
determinants of our wellbeing. The more integrated we are with our community, the less likely we are to experience colds, heart attacks, strikes, cancer, depression and premature death of all sorts.” One of the first to show the association between health and social capi tal was Kawachi, presenting data in which social capital was found to be associated with better health and wellbeing (Kawachi and Kennedy, 1997). Since then, social capital has been found to be associated with a variety of health outcomes (Alvarez et al., 2017; De Silva, 2005; Hawe and Shiell, 2000; Mackenbach et al., 2016; Moore and Kawachi, 2017). In 2017, Moore and Kawachi published a glossary on social capital and health research and highlighted the debates of the definition, measurement and importance of social capi
tal for public health (Moore and Kawachi, 2017). Lately, Alvarez, Kawachi and Romani have suggested that family social capital has a distinct effect on health outcomes (Alvarez et al., 2017). Social capital is now incorporated into the social determinants of health dis course (Carrillo Álvarez and Riera Romaní, 2017). There is a difference between the association of social capital and health and causality; it is not clear to what extent social capital can improve health. In a systematic review Coll-Planas et al. found mixed effects of social capital interventions targeting older people on quality of life, wellbeing and self perceived health (Coll-Planas et al., 2017). In another review on social capital interven tions, the authors concluded that there is a lack of studies that incorporate a multilevel perspective and lack of a more nuanced picture of how social capital can be manipulated to affect health outcomes (Villalonga-Olives et al., 2018). Therefore, further research is needed to understand how social capital can enhance public health.
Future research is also needed to understand the exact mechanism by which social capital may affect health. It is likely that higher levels of social capital result in eco nomic, social, behavioral and emotional benefits that effect health (Burt, 2000; Granovetter, 2005; Welty Peachey et al., 2015). Social capital may enable communities to be more effective at exercising social control over different health behaviors and, therefore, improving the overall wellbeing of the community. In addition, enhanced col lective efficacy and civic engagement to intervene for the common good may help improve health of the individual (Baron-Epel et al., 2008; Berckman and Kawachi, 2014; Carrillo Álvarez and Riera Romaní, 2017; Subramanian, 2002).
Social capital can be measured on the macro level, meso level and individual level (Carrillo Álvarez and Riera Romaní, 2017). Moreover, variations in measurement of social capital are large, and no agreement on how to measure social capital for health research exists; most studies measuring social capital and health look at the community level (Carrillo Álvarez and Riera Romaní, 2017; Mackenbach et al., 2016; Saito et al., 2017; Veenstra et al., 2005).
In other studies, social involvement and social support have been shown to improve wellbeing (Andersen et al., 2019; Bailey et al., 2013). The present study examined if participation in team sports contributed to wellbeing by providing social involvement and social support, over and above the physical activity performed.
The Israeli Cachibol league: Mamanet
The Mamanet League, established in Israel in 2005, is the largest sports organization whose target audience is women, with an emphasis on mothers. The game played in the
6 International Review for the Sociology of Sport 00(0)
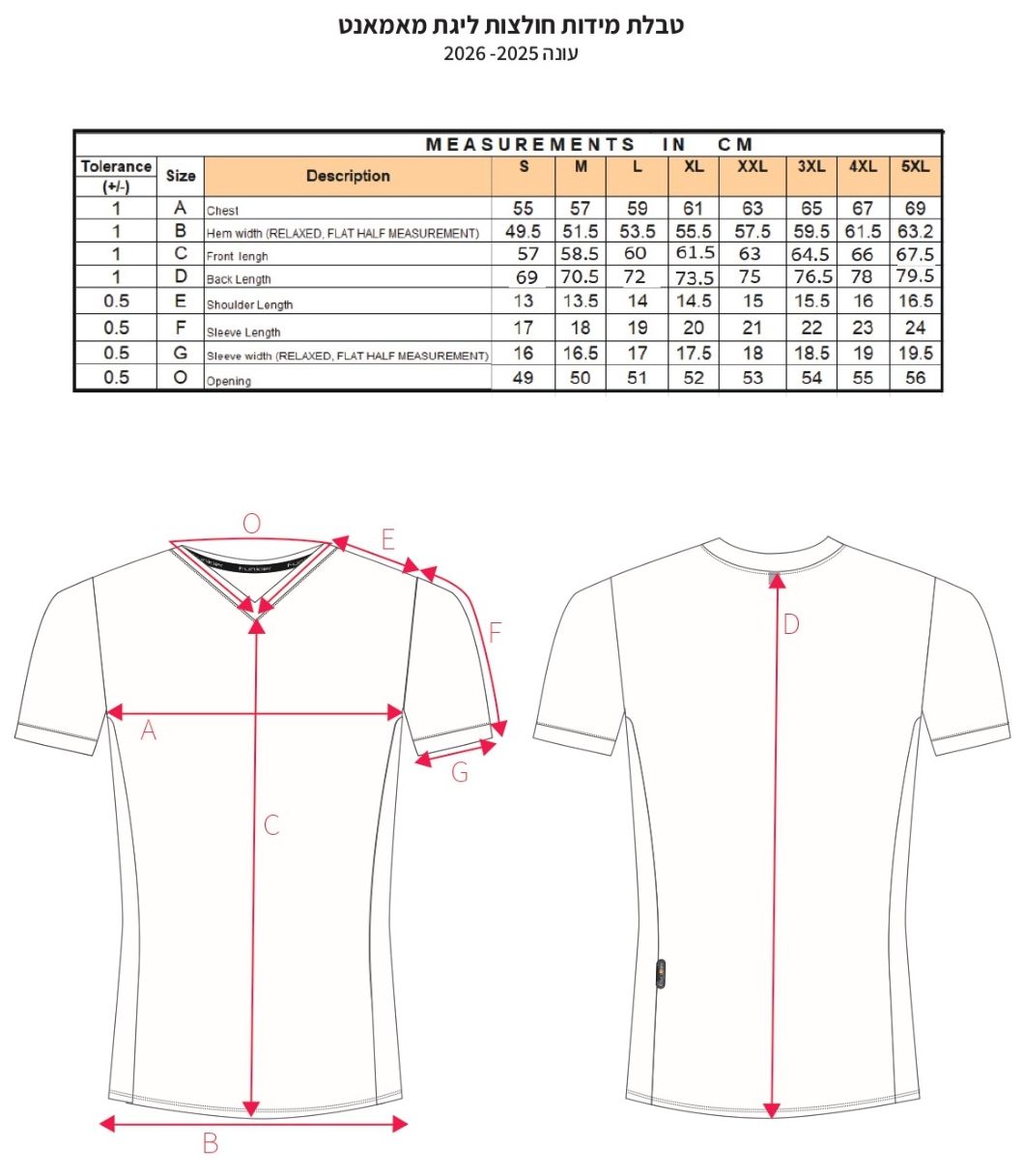
Mamanet League is called “Cachibol” and is also known as “Newcomb ball” (Paul, 1996). The game was invented by Clara Gregory Baer in 1895. Cachibol is a team ball game based on the rules of volleyball and takes place on a court identical to that of vol leyball (9×18 meters). Cachibol and volleyball have the same aim, being to transfer the ball across the net into the opposing court. However, a fundamental difference is that in
cachibol, the players are allowed to catch and hold the ball, not just hit it. The nature of the game allows players of any age or fitness level to be able to learn and participate. Each team consists of up to 14 players, six of whom are on the court at a given time (per team). The objective of the game is to win three-set matches, which are won by achieving 21 points per set. Each set must be won by two points. Points are achieved when the serving team wins the rally. The game is not timed, but generally lasts about 45 minutes. Each team has a coach, a captain, and meets once a week for team practices and once a week for a league game.
Since its establishment, the Mamanet League has spread across Israel and around nine other countries. By 2018, the Israeli Mamanet League included approximately 10,000 players in 800 teams, playing in about 80 leagues throughout the country. The Mamanet League offers “national leagues,” where the teams are based in the child’s school or nearby school. These leagues are open to all mothers and women over 30, with no previ
ous experience needed. In the last few years within this organization new leagues have opened for women over 65 years old, and for fathers and for children. The Mamanet League advocates community involvement and provides a central and important place for social involvement and personal responsibility in the community. The league focuses on sports values and social values, and builds supportive communities around the sports field. The Mamanet League is very active in the social area and community in various ways. For example, members train at-risk youth to be referees for games, and run annual national and international tournaments to raise awareness for breast cancer and much more.
Research questions
Evidence is scarce regarding the effects of participating in sports clubs on various aspects of social life and wellbeing. Therefore, in this study we ask:
(1) Do women participating in the Mamanet League have higher levels of social capital and wellbeing compared with a control group?
(2) Does participation in the Mamanet League improves social capital and wellbeing over time?
Methods
This study is a follow-up study of two groups of mothers: those who participated in the Mamanet League and those who did not participate in any organized sports. Data were collected at two time points. The women were asked to answer the study questionnaire during the first 3 months of joining the league (T1, the end of 2017 to the beginning of 2018), and 13–15 months later (T2, the beginning of 2019). Participants of the control
Baron-Epel et al. 7
group were asked to fill in the study questionnaires at the same time points. The sample of Mamanet players was recruited with the help of the Mamanet organization; the organi zation provided names and phone numbers of the captains, to whom the questionnaire was sent. The captains sent out the online questionnaire via the application WhatsApp. Each team has a WhatsApp group by which they communicate, run by the captain. There was no interaction between the researchers and the women. Those who responded to the
questionnaire at T1 were sent another request to complete the questionnaire at T2. The non-participant control group was recruited from an Internet panel that included 100,000 members. An online questionnaire was sent out to a random sample of women aged 30–50 with at least one child between the ages of 6 and 18. These women reported not participating in any organized competitive sport such as the Mamanet League. Those who responded at T1 answered the questionnaire again at T2. They answered the ques tionnaires at the same time as the Mamanet players. Response rates were 24% for the control group and 33.9% for the Mamanet group.
The study was approved by the ethics committee of the Faculty of Health and Welfare Sciences, University of Haifa.
The Mamanet group included 478 respondents at T1 and 328 respondents at T2. Of the respondents at T1, 124 had dropped out of the teams (37.8%) and for another 10 women we could not match a questionnaire from T1, leaving 194 matched question naires for the intervention group; this amounted to 61.3% loss to follow-up. The control group included 310 respondents at T1 and 122 respondents at T2; loss to follow-up was 60.7%. Analysis was conducted on the data of the 316 women who answered both T1 and the T2 questionnaires.
We conducted a comparison between the respondents and those lost to follow-up and found no significant difference between the groups in age, number of children, body mass index (BMI), marital status, religiosity, or education. The only difference was in family income; the women who dropped out had a lower average income (Z =
3.04, p = .002).
Study variables. The questionnaire included questions about sociodemographic charac teristics, social capital, wellbeing, and health behaviors.
Demographic characteristics included age, number of children, BMI, family and mar ital status, religiosity (secular, religious), education level (academic, non-academic edu cation), and family income (below, average, above average).
Social capital (Onyx and Bullen, 2000); the social capital measure included three indicators: social support, trust, and social involvement. Principal component factor analysis with varimax rotation yielded the following three factors:
- Social support included five items, such as “How many close friends do you have?” and “To what extent do you feel appreciated by society?” Eigenvalue was 3.84, explaining 31.96% of the variance. Loadings ranged between 0.59 and 0.72, and internal consistency was α = 0.74 for T1 and 0.77 for T2.
- Trust included three items, such as “In general, do you think that most people can be trusted, or that you can’t be too careful in dealing with people?” and “In your opinion, would most people try to take advantage of you if given a chance, or
8 International Review for the Sociology of Sport 00(0)
would they try to be fair to you?” Eigenvalue was 1.57, explaining 13.05% of the variance. Loadings ranged between 0.78 and 0.85, and internal consistency was α = 0.82 for T1 and 0.81 for T2. - Social involvement included four items, such as “To what extent have you par ticipated in any community event in the past six months?” and “To what extent are you likely to meet friends or acquaintances when you go out shopping in your area of residence?” Eigenvalue was 1.33, explaining 11.06% of the variance. Loadings ranged between 0.45 and 0.79, and internal consistency was α = 0.64 for T1 and 0.71 for T2.
Scale scores ranged between 1 and 5, with higher scores representing greater social capital. Inter-correlations between the three sub-scales ranged between r = .25 and r = .49 (p < .001), and thus a total score for social capital was composed as well (α = 0.79 for T1 and 0.82 for T2).
Wellbeing variables. Self-reported health (SRH) was measured using the standard ques tion: “How do you evaluate your health generally?” (Baron-Epel and Kaplan, 2001; Kaplan and Baron-Epel, 2003). The scale included six levels, where 6 was excellent and 1 was very bad.
Psychosomatic symptoms were evaluated by the Health Behavior in School-Aged Children checklist, and made up of six items (Hagquist et al., 2019; Haugland and Wold, 2001). Possible items in the checklist included experiencing the following symptoms in the previous 6 months: stomach ache, headache, back ache, irritability or bad temper, feeling low, nervous, dizziness, or difficulty in falling asleep. Answers included: (1) “Rarely or never,” (2) “About every month,” (3) “About every week,” (4) “More than once a week,” and (5) “About every day.” An overall psychosomatic symptom index was created combining all items. Internal consistency was α = 0.73 at T1 and α =0.75 at T2. Higher scores represent a greater extent of symptoms experienced (range 1–5).
Depressive symptoms were based on the Personal and Social Development Survey (Irwin et al., 1999). Respondents were asked to report how frequently during the last week they felt depressed, felt everything they did was an effort, were happy, sleep was restless, lonely and more, all together eight types of feelings. Internal consistency was α
= 0.79 for T1 and α =0.82 for T2. A higher score represented a greater extent of depres sive symptoms (range 1–4). Depressive symptoms scores were computed as a mean score and were log transformed due to non-normal distributions.
Two groups of women answered the questionnaires: the first consisted of mothers who participated in the Mamanet League and the second (control) consisted of mothers who did not participate in group or competitive sports. The women that answered the ques tionnaires had a mean age of 41, with women in the control group being a little younger than the participant group (p = 0.002). There was no significant difference in number of children, BMI, family status, religiosity or family income. However, a higher percent of the control group had a higher education level (p = .045). In both groups the level of
Baron-Epel et al. 9 Table 1. Background characteristics by group, mean or percent (N = 316).
Mamanet participants M (SD)
(n = 194)
Control group
M (SD)
(n = 122)
1–7 2.87 (0.91) 2.82 (0.77) 2.95 (1.10) t(309) = –1.23 (p = .219)
N (%) N (%) N (%)
286 (90.5) 177 (91.2) 109 (89.3) Z = 0.86 (p = .389)
Education Academic 244 (77.2) 142 (74.0) 102 (83.6) Z = 2.00 (p = .045)
196 (62.0) 114 (58.8) 82 (67.2) Z = 1.40 (p = .162)
education was high; between 74% and 83.6% reported having an academic education (Table 1).
Table 2 presents the mean results for the total population (both groups) at T1, as well as the correlations between the variables representing wellbeing and social capital at T1. Generally, social support and SRH were high, and among the social capital components, social involvement had the lowest scores. Depressive symptoms were low. Of the wellbe
ing measures, SRH was not correlated with any of the social capital measures. However, depressive symptoms were significantly correlated with social support, social involve ment and trust (r = –0.40, –0.23, –0.17, respectively), suggesting that the higher the social capital, the lower the depressive symptoms. Psychosomatic symptoms were statisti cally correlated with social support and trust; however, the correlation coefficients were
low (r = –0.14). The three measures of wellbeing were correlated among themselves. An examination of the correlations between the study variables at T1 and the back ground variables revealed significant correlations between age and SRH (r = –.12, p = .033) and age and psychosomatic symptoms (r = –.15, p = .009); no correlation between age and depressive symptoms was observed. Further, education level (academic vs. non academic) and family income (above average vs. average and below average) were asso ciated with “trust” (r = .18, p < .001, r = .11, p = .043 respectively), and family income was associated with depressive symptoms (r = –.13, p = .026). All correlations were weak. As education level and family income are interrelated (r = .38, p < .001), and family income is related to additional study variables compared with education level,
10 International Review for the Sociology of Sport 00(0)
Table 2. Means, standard deviations, and correlations for the study variables at T1 (N = 316). M (SD) 2. 3. 4. 5. 6. 7.
4.10 (0.64) .36*** .46** .81*** .06 –.14* –.40***
4. Total social capital (range of 1–5)
5. Self-reported health (range 1–6)
6. Psychosomatic
symptoms (range of 1–5) 7. Depressive symptoms (range of 1–4)
*p < .05, **p < .01, ***p < .001
2.95 (0.89) 1 .80*** .05 –.09 –.23*** 3.56 (0.59) 1 .07 –.16** –.35*** 5.09 (0.82) 1 –.36*** –.32*** 2.05 (0.66) 1 .48*** 1.62 (0.39) 1
analyses were conducted while controlling for age and family income. In addition, analy ses regarding SRH were conducted while controlling for BMI (r = –.31, p < .001). The results presented in Table 3 show significant group differences at T1. The Mamanet group had higher scores than the control group for the three social capital measures, as well as for SRH. They also had lower scores for psychosomatic symptoms and depressive symptoms compared with the control group.
In light of the initial group differences, change was examined by using group by time interactions, as well as analyzing group differences at T2 while controlling for T1 scores. Age and family income were controlled for. Significant results were found for two of the three social capital measures (social support and social involvement), showing an increase among mothers in the Mamanet group and no change in the control group. No change was found for “trust” in either group.
No change was found regrading SRH. The group by time interactions for psychoso matic symptoms and depressive symptoms were non-significant. However, scores at T2 were lower among Mamanet mothers compared with the control group, even after con trolling for the initial scores.
Multiple hierarchical regressions were calculated to assess the extent to which the background variables and social capital at T1 predict SRH, psychosomatic symptoms and depressive symptoms at T2. Step 1 included group, age, and family income and BMI regarding SRH. Step 2 included the social capital score at T1. Results revealed that 4 of the 5 models were significant. Beyond group, better SRH was related with lower BMI. Experiencing fewer psychosomatic symptoms and lower depressive symptoms were related to higher family income. Further, lower depressive symptoms were related to higher social capital (Table 4).
Next, all continuous variables were standardized and the interaction between group and social capital was defined. This was entered in the third step of each regression
Baron-Epel et al. 11
symptoms
Step 1
Self-reported health
Psychosomatic symptoms
Group .22*** –.27*** –.23*** Age –.10 –.09 .05 Family income .08 –.14** –.13* BMI –.25*** – – Social capital .05 –.09 –.33***
Adj.R2 .114*** .119*** .202*** F(4, 311) 9.08*** 11.59*** 20.98***
*p<.05, **p<.01, ***p<.001. Note. Group: 1, Mamanet, 0, control. Family income: 1, above average, 0, average and below. For self-reported health df = 5, 310.
BMI: body mass index.
model. The interaction was found significant regarding psychosomatic symptoms (β = .18, p = .031), adding 1.0% to the explained variance (p = .031). Its interpretation with simple slopes (Dawson, 2014; Toothaker et al., 1994) revealed a negative relationship between social capital and psychosomatic symptoms for the control group (Coefficient = –0.16, t = –2.73, p = .007), and a non-significant relationship for the Mamanet group (Coefficient = 0.01, t = 0.12, p = .903). This suggests that women in the control group who had higher social capital levels reported lower levels of psychosomatic symptoms, this not being apparent in the Mamanet group.
The interaction between group and social capital was not significant regarding SRH (β = .08, p = .317), nor was it significant regarding depressive symptoms (β = .11, p = .180).
Our first research question was related to the initial differences in social capital and well being between women participating in the Mamanet League and those not participating. Do participants in a sports team have higher levels of social capital and wellbeing com pared with non-participants to begin with? Our findings suggest that women participat ing in the league have higher levels of social capital when joining the team, compared with women not joining the team (the control group). All three measures of social capital were higher at the beginning of the study among the team participants: social support,
Baron-Epel et al. 13
trust and social involvement. As Mamanet participation is voluntary and demands intense active participation, it was not expected that the two groups would be similar, as only women with high motivation and interest in participating in competitive sports typically join the team. The recruitment of participants to the Mamanet League is based on them having children in elementary school. This already defines a subset of mothers connected to the school setting. Women were often recruited to Mamanet via other mothers at their children’s schools, suggesting these women were already socially connected to other mothers in the neighborhoods and schools. This is in line with the concept of social capi tal where people with higher levels of social capital are able to utilize resources in the community in order to benefit themselves (Putnam, 2000). It is often assumed that mem
bership in voluntary associations increases social capital; however, it may be the other way round: positive correlations between civic participation and trust are at least partly caused by self-selection of trusting citizens into associations (Sønderskov, 2011). These women self-select for participation in the league.
In addition to having higher levels of social capital when joining the league, these women also seem to exhibit better health and wellbeing at that point. Women joining the teams in the league had higher levels of wellbeing for all three measures: SRH was better among Mamanet participants, and psychosomatic and depressive symptoms were lower compared with women not joining the league. This might suggest that this type of physi
cal and social activity is not attractive to all women equally, and that women with higher levels of wellbeing may be more attracted to join in the games, again self-selecting. This is backed by the high level of dropout observed, suggesting it is suitable for a small seg ment of the population; most women may not enjoy both competitive sports and intense social interactions that are characteristic of sports teams, or cannot find time within their schedules for these activities. Most of these mothers have small children, and the games take place in the late evening, therefore they are expected to leave their families for a few hours at least twice a week. This kind of investment in themselves is not an easy task, therefore only healthy women and women socially integrated in the local community and with high levels of social support will join in.
Our second research question was: does participation in the Mamanet League improve social capital and wellbeing? Social support and social involvement, but not trust, improved during the year of follow-up, from initially joining the league to a year later. No such changes were observed for the control group of non-participant women. It seems that participation in the Mamanet League increased women’s social capital regarding certain aspects of it, although the change was small. A longer duration of follow-up may enable observation of larger changes in social capital.
The increase in reported social support and involvement may be a result of increased social interactions and an extended social network. Women joining in the league attend practice sessions and games, get to know women they did not know before and get involved in other social activities that commonly take place within the team; this obvi
ously adds to their exposure to the community in which they live. These activities in which the women were involved do not necessarily increase trust, as they only involved a specific group of mothers and few interactions took place with other individuals from other realms of society. So, while no increase in trust was reported after a year of partici
pation, it is again possible that a longer follow-up period would yield different findings.
14 International Review for the Sociology of Sport 00(0)
Increase in social capital can also result from the actual involvement in competitive sports and may not only be due to social interactions. However, in this study we cannot differentiate between the sports activities and the social activities involved in the partici pation in the league. Theoretically, the type of social capital that is studied here is bond ing social capital, as these women are more or less from a homogeneous group of mothers living in neighborhoods near the elementary school to which their children go to school and where the team practices. No measure of bridging or linking social capital was meas ured in this study. The increase in social capital observed may be due both to the social aspects of belonging to the team and to the competitiveness of the game.
In the literature, it was initially suggested by Putnam (2000), and discussed more recently by Lewandowski (2018), that sports could be a mechanism for the production of general trust and social capital. The present study suggests that when joining a competi tive sports group, only social support and social involvement improve over time, but trust does not necessarily improve. Lewandowski (2018) suggests that sport does not produce trust, but rather reinforces the existing trust; we suggest that trust in our study was com paratively high and therefore no change could be identified due to a ceiling effect. Coalter (2007) explored the contribution of sports clubs to the development of social capital and concluded that it was not clear what role sports clubs can play. A study in Denmark and the Netherlands reported that duration of membership and membership participation in sports clubs did not impact social trust, similar to our findings (Elmose-Østerlund and van der Roest, 2017). The authors suggest that higher levels of trust cannot be attributed to the participation in the clubs. A study in Germany looking at sports clubs among other civic associations suggests that the social capital-generating effects of sports clubs may have weakened over time, from 2001 to 2017/18 (Burrmann et al., 2019).
A qualitative study of young immigrant women in Norway participating in team sports revealed that participation in team physical activity evoked feelings of camaraderie and community, although the connections formed were described as acquaintances rather than those of friends. The women in the study further reported that they more easily connected with other individuals of an immigrant background, rather than with native Norwegians, often due to socioeconomic differences between the two groups (Walseth, 2008). In another study in India, Kay (2009) studied adolescent girls participating in a sports-for-development program; they showed an increase in social connections and confidence among the partici pants, indicating an increase in social capital as a result of participation in group sports.
All in all, some studies, but not all, support the idea that participation in sports clubs may increase social capital; our study suggests social support and involvement, but not trust, improve when joining the team. However, the assumption that belonging to a sports club can improve social capital depends on context and population, and cannot be gener
alized to all populations and settings.
Social capital is an umbrella concept that includes both cognitive and structural aspects. Five different indicators were suggested by Putnam to form the social capital concept, as described in the introduction. One of them was trust. The fact that trust was not found to change in this study, when the other two indicators did change, suggests that maybe, theoretically, the umbrella concept depends on the population and situation at hand and cannot be generalized to all settings. Such broad concepts such as social capital often are too broad to “fit all.” Maybe a more modular approach needs to be adopted, in
Baron-Epel et al. 15
which various indicators describe the concept of social capital in more specific settings and not all five indicators are relevant simultaneously for all settings. It is possible that a community-based sports league might serve as a social anchor for those individuals and families participating in these sports leagues (Clopton and Finch, 2011). Mamanet, a league based around the elementary school system, might benefit from a social anchor theory analysis. Social anchor theory examines institutions that support the development and preservation of social capital and networks at the community level and provide a sense of cohesiveness for the collective identity of that community (Clopton and Finch, 2011). As such, the Mamanet League may serve to develop and maintain social capi tal and networks at the community level and increase collective identity of the community. Mamanet may provide some form of uniqueness or identity for community members. Our second research question included, in addition to social capital, the question of changes in health and wellbeing as a result of joining the league. The improvement in health could be due to the social or the sports part of the activities; we cannot differenti ate between them. After more than a year follow-up, there were no significant changes in wellbeing (SRH, psychosomatic symptoms and depressive symptoms) among the women in either group. As the duration of the follow-up period was only 1 year, this may serve as too short a period for changes in wellbeing to be expressed in a self-reported survey at this comparatively young age. In the control group, the changes were also non-signifi cant. Longer follow-up studies are needed to observe possible changes in wellbeing com pared with the control. Other studies have found such relationships; for example, Guimaras and Baptista (2011) studied women during menopause participating in team sports and found improvements in the wellbeing of participants, social relationships, social support and sexual activity. Social capital has been shown to be associated with various types of health measures, and in some cases to serve as a predictor of health (Glanville and Story, 2018). For example, research has shown that social integration can enhance population wellbeing (McNeill et al., 2006).
Two reviews looked at interventions that assessed if social capital can improve health, and mixed results were reported (Coll-Planas et al., 2017; Villalonga-Olives et al., 2018). Our study does not support the hypotheses that joining the team can improve health.
Although the research questions did not include analyzing the association between social capital and health, we do find the association between social capital and health worth reporting.
Social capital, at the time of joining the team, was associated with wellbeing a year later; this suggests a unidirectional relationship, where higher social capital may predict fewer depressive symptoms a year later, but not SRH or psychosomatic symptoms. Each type of wellbeing represents a different aspect of health and wellbeing: SRH and psycho
somatic symptoms serve more as a measure of physical health, whereas depressive symptoms are more a measure of mental health. Mental health may not be related as strongly with age as is physical health, therefore in this relatively young group of women, only mental health may be largely affected by social variables such as social capital.
When analyzing the interactions between the groups we found that among the con trols, women with higher initial social capital reported lower levels of psychosomatic symptoms a year later. Among the women participating in the league this association was not observed. This difference between the groups suggests that participation in the league
16 International Review for the Sociology of Sport 00(0)
may protect from the ill effects of low social capital regarding psychosomatic symptoms. We would expect to find this association between social capital and all health measures in both groups. The fact that this was not observed for all wellbeing measures may be due to the homogeneous study population including women with comparatively high levels of social capital, education, and socioeconomic status. To further study the possibility that joining the league could improve social capital and wellbeing, future studies should include women from lower socioeconomic status backgrounds.
The present study suggests that interventions including physical activity and social interactions among women can benefit women: obviously for increased engagement in physical activity, as well as for the benefits of improving their social support and social involvement in the community. This increase in social capital may provide benefits that will be demonstrated as health benefits, mainly mental health benefits, after longer peri
ods than tested in this study.
This study cannot differentiate between the social, competitive and physical activity aspects of belonging to the Mamanet League. We cannot differentiate between perform ing physical activity or joining a team as a factor influencing social capital. The fact that there is no change in social capital in the control group with time suggests that joining the sport team does increase social capital.
The strength of this study is in its 13–15-month follow-up design, enabling analysis of changes occurring in a group of mothers playing in the league when compared with women who are not active in such a team (the controls).
However, a year of follow-up may not be long enough to provide evidence of change in health and trust in these young, healthy and connected women.
This was not an intervention with a random assignment of women to control and intervention groups, therefore the differences between the intervention and control group may interfere with the observations and conclusions. However, testing these measures in real life can also add to our knowledge, as it is clear that this type of sport is not suitable for all women, and only women with an interest in competitive group sport will self
select and join.
The study also suffered loss to follow-up; however, the difference between those who did and did not answer the questionnaire was only regarding income, and the regression models adjusted for this. The dropout of women from the team does suggest this activity does not suit all young mothers, and further development of interventions to get women to be active is needed.
Putnam’s theory of social capital suggests that participation in spots teams can foster social capital and health. This study suggests partial support for the theory; social sup port and social involvement do increase when attending a women’s sports team. However, trust and health and wellbeing do not increase a year after joining the team.
Baron-Epel et al. 17
We would like to thank all the Mamanet players that participated in the study and the Mamanet organization for helping in requirement of participants.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) disclosed receipt of the following financial support for the research, authorship, and/ or publication of this article: Ministry of Science, Technology and Space, Israel.
Orna Baron-Epel https://orcid.org/0000-0003-3447-2594
Alvarez EC, Kawachi I and Romani JR (2017) Family social capital and health – A systematic review and redirection. Sociology of Health and Illness 39(1): 5–29.
Andersen MH, Ottesen L and Thing LF (2019) The social and psychological health outcomes of team sport participation in adults: An integrative review of research. Scandinavian Journal of Public Health 47(8): 832–850.
Bailey R, Hillman C, Arent S, et al. (2013) Physical activity: An underestimated investment in human capital? Journal of Physical Activity and Health 10(3): 289–308.
Ball K, Cleland VJ, Timperio AF, et al. (2010) Love thy neighbour? Associations of social capi tal and crime with physical activity amongst women. Social Science and Medicine 71(4): 807–814.
Baron S, Field J and Schuller T (2000) Social Capital: Critical Perspectives. Oxford: Oxford University Press.
Baron-Epel O and Kaplan G (2001) General subjective health status or age-related subjective health status: Does it make a difference? Social Science & Medicine 53(10): 1373–1381. Baron-Epel O, Weinstein R, Haviv-Mesika A, et al. (2008) Individual-level analysis of social
capital and health: A comparison of Arab and Jewish Israelis. Social Science and Medicine 66(4): 900–910.
Bartkus V and Davis J (2010) Social capital: Reaching out, reaching in. Available at: https:// books.google.com/books?hl=en&lr=&id=KUj4cjvxUX8C&oi=fnd&pg=PR1&dq=Bartkus +and+Davis,+2009&ots=eI_BdIIIQR&sig=-G_VqgzOnYqBZYtEojdPl6shJLE (accessed 22 June 2020).
Berckman LF and Kawachi IGM (ed.) (2014) Social Epidemiology. 2nd ed. Oxford: Oxford University Press.
Bourdieu P (1984) Distinction. London: RKP.
Bourdieu P (1986) The forms of capital. In: Richards JR (ed.) Handbook of Theory and Research for the Sociology of Education. New York: Greenwood Press, pp. 241–258. Burnett C (2006) Building social capital through an ‘active community club’. International Review for the Sociology of Sport 41(3–4): 283–294.
18 International Review for the Sociology of Sport 00(0)
Burrmann U, Braun S and Mutz M (2019) Playing together or bowling alone? Social capital related attitudes of sports club members and non-members in Germany in 2001 and 2018. European Journal for Sport and Society 16(2): 164–186.
Burt RS (2000) The network structure of social capital. Research in Organizational Behavior 22: 345–423.
Carrillo Álvarez E and Riera Romaní J (2017) Measuring social capital: Further insights. Gaceta Sanitaria 31(1): 57–61.
Clopton A (2012) Social capital, gender, and the student athlete. Group Dynamics: Theory, Research, and Practice 16(4): 272–288. Available at: https://psycnet.apa.org/record/2012-23733-001 (accessed 16 June 2020).
Clopton AW and Finch BL (2011) Re-conceptualizing social anchors in community develop ment: Utilizing social anchor theory to create social capital’s third dimension. Community Development 42(1): 70–83.
Coalter F (2007) Sports clubs, social capital and social regeneration: ‘ill-defined interventions with hard to follow outcomes’? Sport in Society 10(4): 537–559.
Coleman JS (1988) Social capital in the creation of human capital. American Journal of Sociology 94: S95–S120.
Coleman JS (1990) Equality and Achiement in Education. Boulder CO: West View Press. Coll-Planas L, Nyqvist F, Puig T, et al. (2017) Social capital interventions targeting older people and their impact on health: A systematic review. Journal of Epidemiology and Community Health 71: 663–672.
Dawson JF (2014) Moderation in management research: What, why, when, and how. Journal of Business and Psychology 29(1): 1–19.
De Silva MJ (2005) Social capital and mental illness: A systematic review. Journal of Epidemiology & Community Health 59(8): 619–627.
Elmose-Østerlund K and van der Roest JW (2017) Understanding social capital in sports clubs: Participation, duration and social trust. European Journal for Sport and Society 14(4): 366–386. Feldstein L and Putnam R (2003) Better Together. New York: Simon & Schuster. Ferlander S, Stickley A, Kislitsyna O, et al. (2016) Social capital-a mixed blessing for women? A cross-sectional study of different forms of social relations and self-rated depression in Moscow. BMC Psychology 4(1): 37.
Field J (2003) Social Capital. London: Routledge.
Forsdike K, Marjoribanks T and Sawyer AM (2019) ‘Hockey becomes like a family in itself’: Re-examining social capital through women’s experiences of a sport club undergoing quasi professionalisation. International Review for the Sociology of Sport 54(4): 479–494.
Gidengil E and O’Neill BL (2006) Removing rose colored glasses. In: Gender and Social Capital, pp. 1–14. Available at: https://books.google.com/books?hl=en&lr=&id=UuV5xzkOkygC& oi=fnd&pg=PA1&dq=Gidengil+2006&ots=Esw8Ji755f&sig=FgjPWz6Czuqbo-0uBGpkFv Xl4c4 (accessed 22 June 2020).
Glanville JL and Story WT (2018) Social capital and self-rated health: Clarifying the role of trust. Social Science Research 71: 98–108.
Granovetter M (2005) The impact of social structure on economic outcomes. Journal of Economic Perspectives 19(1): 33–50.
Guimarães ACA and Baptista F (2011) Influence of habitual physical activity on the symptoms of climacterium/menopause and the quality of life of middle-aged women. International Journal of Women’s Health 3(1): 319–328.
Hagquist C, Due P, Torsheim T, et al. (2019) Cross-country comparisons of trends in adolescent psychosomatic symptoms – A Rasch analysis of HBSC data from four Nordic countries. Health and Quality of Life Outcomes 17(1): 27.
Baron-Epel et al. 19
Harpham T (2002) Measuring social capital within health surveys: Key issues. Health Policy and Planning 17(1): 106–111.
Harvey J, Lévesque M and Donnelly P (2007) Sport volunteerism and social capital. Sociology of Sport Journal 24(2): 206–223.
Haugland S and Wold B (2001) Subjective health complaints in adolescence—Reliability and validity of survey methods. Journal of Adolescence 24(5): 611–624.
Hawe P and Shiell A (2000) Social capital and health promotion: A review. Social Science & Medicine 51(6): 871–885.
Irwin M, Artin KH and Oxman MN (1999) Screening for depression in the older adult. Archives of Internal Medicine 159(15): 1701.
Jarvie G (2003) Communitarianism, sport and social capital. International Review for the Sociology of Sport 38(2): 139–153.
Johnston G and Percy-Smith J (2003) In Search of Social Capital. Policy & Politics. London: Routledge.
Kaplan G and Baron-Epel O (2003) What lies behind the subjective evaluation of health status? Social Science & Medicine 56(8): 1669–1676.
Kawachi I and Kennedy BP (1997) Socioeconomic determinants of health: Health and social cohe sion: Why care about income inequality? BMJ 314(7086): 1037.
Kay T (2009) Developing through sport: Evidencing sport impacts on young people. Sport in Society 12(9): 1177–1191.
Lewandowski JD (2015) Capitalising sociability: Rethinking the theory of social capital. In: Edwards R, Franklin J and Holland J (eds) Assessing Social Capital: Concept, Policy and Practice. Newcastle, NE: Cambridge Scholars Press, pp. 14–28.
Lewandowski JD (2018) Sport, trust, and social capital. Comparative Sociology 17(3–4): 386–405. Mackenbach JD, Lakerveld J, van Lenthe FJ, et al. (2016) Neighbourhood social capital: Measurement issues and associations with health outcomes. Obesity Reviews 17: 96–107. McNeill LH, Kreuter MW and Subramanian SV (2006) Social environment and physical activity: A review of concepts and evidence. Social Science and Medicine 63(4): 1011–1022. Marlier M, Van Dyck D, Cardon G, et al. (2015): Interrelation of sport participation, physical activity, social capital and mental health in disadvantaged communities: A SEM-analysis. PLoS ONE 10: e0140196.
Moore S and Kawachi I (2017) Twenty years of social capital and health research: A glossary. Journal of Epidemiology and Community Health 71(5): 513–517.
Numerato D (2008) Czech sport governing bodies and social capital. International Review for the Sociology of Sport 43(1): 21–34.
Okayasu I, Kawahara Y and Nogawa H (2010) The relationship between community sport clubs and social capital in Japan: A comparative study between the comprehensive community sport clubs and the traditional community sports clubs. International Review for the Sociology of Sport 45(2): 163–186.
Onyx J and Bullen P (2000) Measuring social capital in five communities. The Journal of Applied Behavioral Science 36(1): 23–42.
Osborne K, Baum F and Ziersch A (2009) Negative consequences of community group participa tion for women’s mental health and well-being: Implications for gender aware social capital building. Journal of Community and Applied Social Psychology 19(3): 212–224.
Ottesen L, Jeppesen RS and Krustrup BR (2010) The development of social capital through football and running: Studying an intervention program for inactive women. Scandinavian Journal of Medicine & Science in Sports 20: 118–131.
Pahl R (2000) On Friendshipno Title. Cambridge: Polity Press.
20 International Review for the Sociology of Sport 00(0)
Paul J (1996) A lost sport : Clara Gregory Baer and Newcomb ball. Journal of Sport History 23(2): 165–174. Available at: https://www.jstor.org/stable/43609991 (accessed 16 June 2020). Perks T (2007) Does sport foster social capital? The contribution of sport to a lifestyle of commu nity participation. Sociology of Sport Journal 24(4): 378–401.
Putnam RD (1993) Making Democracy Work. Princeton, NJ: Princeton University Press. Putnam RD (1995) Bowling alone: America’s declining social capital. Journal of Democracy 6: 65–78.
Putnam RD (1996) The strange disappearance of civic America. The American Prospect 24: 34–48. Available at: https://search.informit.com.au/fullText;dn=970201788;res=IELAPA (accessed 23 June 2020).
Putnam RD (2000) Bowling alone: The collapse and revival of American community. Available at: https://www.google.com/books?hl=en&lr=&id=rd2ibodep7UC&oi=fnd&pg=PA13&dq- =putnam+bowling+alone&ots=G5KfoVskW1&sig=8n2i6803Q-BDnExivwi5AprnFP4 (accessed 5 January 2020).
Sønderskov KM (2011) Does generalized social trust lead to associational membership? unravel ling a bowl of well-tossed Spaghetti. European Sociological Review 27(4): 419–434. Saito M, Kondo N, Aida J, et al. (2017) Development of an instrument for community-level health related social capital among Japanese older people: The JAGES project. Journal of Epidemiology 27(5): 221–227.
Seippel Ø (2006) Sport and social capital. Acta Sociologica 49(2): 169–183. Sherry E (2010) (Re)engaging marginalized groups through sport: The homeless World Cup. International Review for the Sociology of Sport 45(1): 59–71.
Sherry E, Karg A and O’May F (2011) Social capital and sport events: Spectator attitudinal change and the homeless world cup. Sport in Society 14(1): 111–125.
Smith ACT and Westerbeek HM (2014) Sport as a vehicle for deploying corporate social respon sibility. Journal of Corporate Citizenship 2007(25): 43–54.
Spaaij R (2009) Sport as a vehicle for social mobility and regulation of disadvantaged urban youth: Lessons from Rotterdam. International Review for the Sociology of Sport 44(2–3): 247–264. Subramanian SV (2002) Social trust and self-rated health in US Communities: A multilevel analy sis. Journal of Urban Health: Bulletin of the New York Academy of Medicine 79(90001): 21S–34.
Toothaker LE, Aiken LS and West SG (1994) Multiple regression: Testing and interpreting inter actions. The Journal of the Operational Research Society 45(1): 119.
Veenstra G, Luginaah I, Wakefield S, et al. (2005) Who you know, where you live: Social capital, neighbourhood and health. Social Science & Medicine 60(12): 2799–2818. Villalonga-Olives E, Wind TR and Kawachi I (2018) Social capital interventions in public health: A systematic review. Social Science and Medicine 212: 203–218.
Walseth K (2008) Bridging and bonding social capital in sport—experiences of young women with an immigrant background. Sport, Education and Society 13(1): 1–17. Welty Peachey J, Borland J, Lobpries J, et al. (2015) Managing impact: Leveraging sacred spaces and community celebration to maximize social capital at a sport-for-development event. Sport Management Review 18(1): 86–98.
Welty Peachey J, Cohen A, Borland J, et al. (2013) Building social capital: Examining the impact of Street Soccer USA on its volunteers. International Review for the Sociology of Sport 48(1): 20–37.